Did you know that ischemic heart disease accounts for 13% of all global fatalities? According to World Health Organization data collected between 2000 and 2021, this single category causes more deaths than almost any other condition on the planet. You likely hear terms like Coronary Artery Disease isthe leading cause of death globally due to the narrowing or blockage of coronary arteries caused by plaque buildup.CAD, commonly known as heart disease, affects millions of adults in the United States alone. If you have been diagnosed with this condition, or if you are worried about family history, understanding exactly what happens inside your chest can empower your decisions. We often treat symptoms without addressing the root cause, so let us look past the chest pain and examine the actual mechanics of the disease.
The Mechanics of Atherosclerosis: More Than Just Clogging
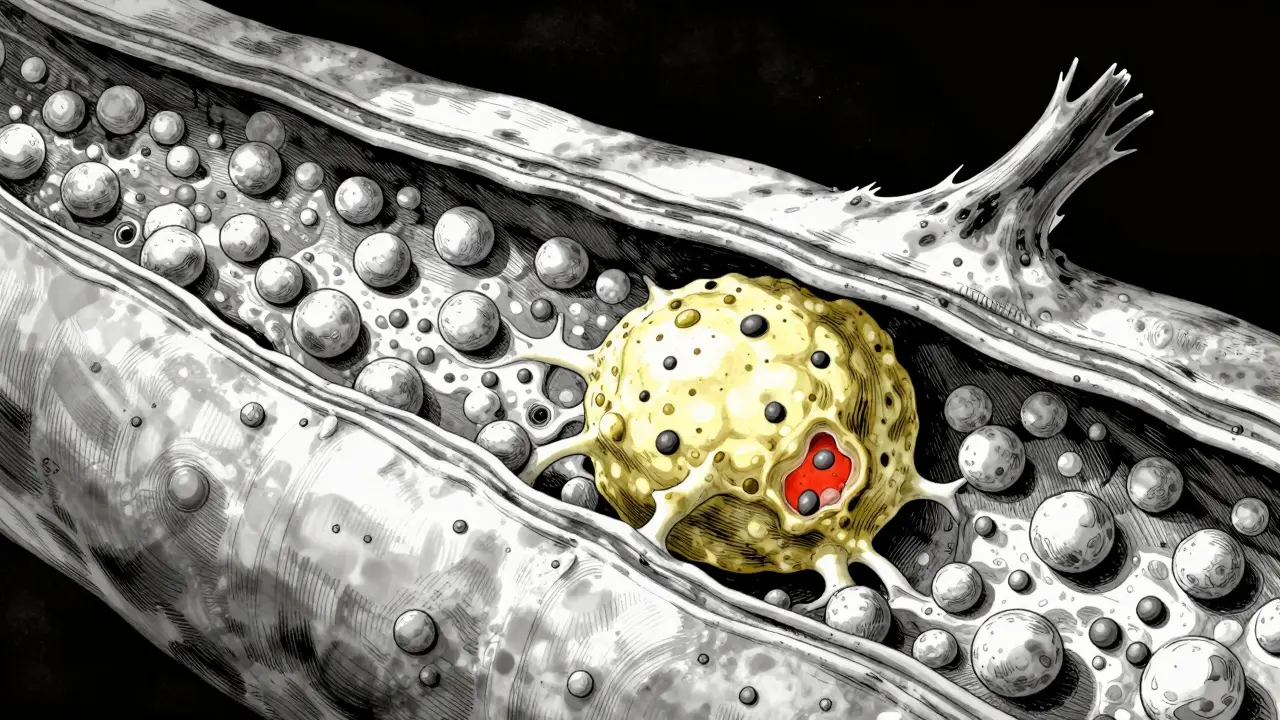
You might imagine your arteries as garden hoses getting stiff with age, but the reality of Atherosclerosisa complex chronic inflammatory condition involving the accumulation of fatty deposits, cholesterol, and other substances within the arterial wall is far more intricate. It starts at a microscopic level. Endothelial dysfunction occurs first, where the inner lining of the blood vessel gets damaged. This damage often comes from high blood pressure or tobacco smoke irritation. Once the lining is compromised, low-density lipoprotein (LDL) particles begin to infiltrate the arterial wall.
These LDL particles oxidize, triggering an immune response. White blood cells called macrophages rush to the site to clean up the mess, but instead of clearing it away, they transform into foam cells. This creates a fatty streak that eventually evolves into a full-blown plaque. The composition matters immensely. Unstable plaques typically have a high macrophage content, a thick lipid core, and a very thin fibrous cap. Surprisingly, these dangerous plaques often narrow the vessel lumen by less than 50%. Conversely, a stable plaque might have a thicker cap and fewer lipids, causing significant narrowing but being less prone to rupture.
This distinction is vital because a sudden heart attack often comes from an unstable plaque rupturing rather than a slowly closing tube. When a thin-capped plaque bursts, the body reacts by forming a clot right there to heal the breach. This clot can abruptly cut off oxygen to the heart muscle. Understanding this biology helps explain why some people get heart attacks seemingly out of nowhere, even if their arteries didn't look fully blocked on previous imaging tests.
Identifying Your Personal Risk Profile
Not everyone faces the same threat level. Medical professionals use sophisticated models to categorize patients into Low, Intermediate, or High risk. The American College of Cardiology and the American Heart Association (ACC/AHA) utilize a yearly risk prediction system. Here is how the math works:
- Low Risk: Less than 1% chance of cardiovascular death or nonfatal myocardial infarction per year.
- Intermediate Risk: Between 1% and 3% annual probability.
- High Risk: Greater than 3% annual probability.
If you fall into the high-risk bucket, your treatment plan changes significantly. Research indicates that 60% of the total patient population exhibits high-risk features. This group includes people with involvement of two or more vascular beds, such as having both carotid and leg artery disease alongside heart issues. Other high-risk markers include a history of heart failure with preserved ejection fraction, a kidney function marked by an estimated glomerular filtration rate (eGFR) below 60 ml/min, or a diagnosis of diabetes.
Social and lifestyle factors also weigh heavily here. Smoking status is a massive variable. Even if you quit years ago, the lingering damage to endothelial health persists longer than many realize. Body Mass Index (BMI) is another tracked metric. Elevated BMI correlates strongly with metabolic syndrome, which drives up blood pressure and cholesterol simultaneously. While genetics play a role, modifiable factors like diet, exercise, and smoking habits offer a way to shift your risk category downward.
How Diagnosis Happens in Modern Medicine
When you feel chest tightness or shortness of breath, doctors need to rule out other causes before confirming CAD. The journey usually begins with a simple electrocardiogram (ECG). This test records the electrical signals firing through your heart to identify arrhythmias or signs of past damage. However, an ECG at rest might look normal even if you have significant blockages. That is why stress testing is often the next step. You walk on a treadmill or use a bicycle ergometer while monitors track your heart rate and electrical activity under physical exertion.
| Test Name | Primary Purpose | Invasiveness Level |
|---|---|---|
| Electrocardiogram (ECG) | Check heart rhythm and electrical conduction | Non-invasive |
| Stress Test | Evaluate heart response to physical activity | Non-invasive |
| Coronary Angiography | Visualize blockages using contrast dye | Invasive |
| Ankle-Brachial Index | Diagnose peripheral artery disease coexistence | Non-invasive |
If initial screening suggests obstruction, coronary angiography becomes the gold standard. This procedure involves threading a catheter through an artery in your wrist or groin up to the heart. The doctor injects contrast dye and uses X-rays to see exactly where the flow slows down. Recently, clinicians also recommend the Ankle-Brachial Index (ABI). Since Peripheral Artery Disease (PAD) frequently coexists with CAD, checking the ratio of blood pressure at your ankle compared to your arm gives clues about systemic vascular health throughout your body.
Treatment Strategies: From Pills to Surgeries
Once the diagnosis lands, the goal shifts to stabilizing the plaque and restoring blood flow. Treatment is rarely a one-size-fits-all approach. Your cardiologist will look at your specific anatomy and overall health profile. Pharmacotherapy remains the foundation of management. Statin therapy is the most common first-line defense. These drugs work by inhibiting the production of cholesterol in the liver and lowering LDL levels in the blood.
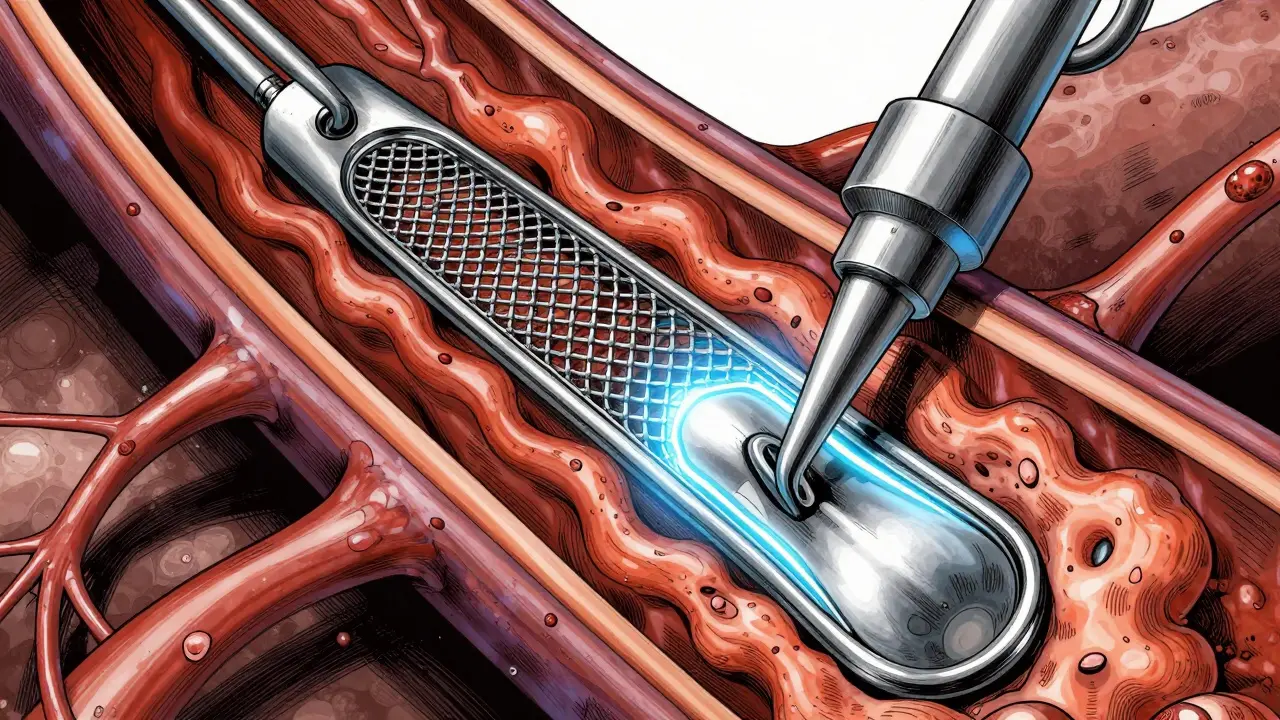
However, sometimes medication cannot clear a critical blockage fast enough. In cases of severe stenosis, revascularization procedures are necessary. Percutaneous Coronary Intervention (PCI) is the most common method. During PCI, a balloon inflates inside the narrowed artery to compress the plaque against the wall, followed by the placement of a stent-a small mesh tube-to keep the artery open. This is minimally invasive and allows for a relatively quick recovery.
For complex cases where multiple arteries are blocked, or the anatomy is too difficult for stenting, Coronary Artery Bypass Grafting (CABG) is the option. Surgeons take a healthy blood vessel from your chest or leg and graft it onto the coronary artery, creating a new path around the blockage. This major surgery carries higher risks but offers durable results for complicated heart disease.
Life With Chronic Coronary Disease
Living with CAD is a long-term commitment, but it does not mean you cannot enjoy a full life. Patients who have suffered acute heart attacks or experience chest angina require lifelong medication management, though dosages may change over time based on clinical response. It is also important to recognize that as populations age, patients increasingly suffer from concurrent conditions. Cancer survival rates are improving, meaning more people live long enough to develop heart issues. This intersection has birthed cardio-oncology, a specialized field managing patients with both cancer and heart disease.
Dr. Christopher B. Granger, lead author of the 2023 ACC/AHA guidelines, emphasized that risk stratification is fundamental. He notes that therapy intensity must match the 1% to 3% risk classification system. Whether you are taking aspirin daily or preparing for a bypass, personalized therapeutic strategies optimize outcomes. The economic burden of this care is substantial, with projected annual costs reaching $1.1 trillion by 2035. Investing in prevention and early detection isn't just personal; it is a societal necessity.
Can Coronary Artery Disease be reversed completely?
While you cannot entirely remove hardened calcium plaques, aggressive lifestyle changes and medications can stabilize existing plaque and prevent further progression. Some studies suggest modest regression of soft plaque components is possible with strict adherence to diet and statin therapy.
What is the difference between stable and unstable angina?
Stable angina occurs predictably during physical exertion and resolves with rest, indicating fixed blockages. Unstable angina happens unpredictably, even at rest, signaling a rupture-prone plaque requiring immediate medical intervention.
Do I need an angiogram before starting medication?
Not necessarily. Many patients start risk-factor modification therapies like statins based on risk calculators alone. Angiography is reserved for those with positive stress tests or high-grade symptoms suggesting imminent danger.
How does smoking affect my CAD risk specifically?
Smoking damages the endothelium, making it easier for LDL to enter artery walls. Quitting reduces inflammation rapidly, but the risk remains elevated for years compared to someone who never smoked.
Is PCI better than bypass surgery?
It depends on complexity. PCI is preferred for simpler, single-vessel disease due to faster recovery. Bypass is better for multi-vessel disease or diabetic patients, offering longer-term patency of the blood vessels.





Rohan Kumar
28 March 2026 - 16:17 PM
Another day another study saying eat less fat while selling us processed garbage 🙄. The statistics look nice on paper but ignore the real world toxicity everywhere. Everyone knows the blood banks profit more than doctors admit publicly. We see the patterns hiding behind the jargon terms like endothelial dysfunction. Just keep taking the pills until you need a bypass surgery 😒.
Aaron Olney
28 March 2026 - 20:55 PM
my dad died from this last year and it was horrable i still remember the hospital screaming. he was fine one minite then his heart just stopped working completly. doctors said the plaque broke open but it felt so sudden and unfair. we were told he was healthy because his tests looked normal before. nobody tells you the scary parts of how arteries get blocked like this. i wake up thinking about the angiogram machine and how cold the room was. it changes your whole perspective on what you put in your mouth every day now. smoking killed him even though he quit years ago apparently.
Rachael Hammond
30 March 2026 - 05:22 AM
the concept of foam cells transforming the arterial wall is really interesting to me personally. we dont think enough about inflammation causing damage before the clog appears. maybe focusing on reducing stress would help heal the lining better. i read somewhere that anger increases bad particles in the blood stream quickly. its like our emotions physically change the vessels inside us over time. there is a deeper connection between mental state and physical plaque buildup. understanding this makes prevention feel more possible than just taking pills alone.
Sabrina Herciu
31 March 2026 - 06:43 AM
Statin therapy remains the primary defense mechanism for most patients today. These drugs inhibit cholesterol production within the liver effectively. Lowering LDL levels becomes the immediate clinical goal for everyone involved. Plaque stabilization occurs when inflammatory markers drop significantly over time. Rupture events diminish drastically once the fibrous cap thickens appropriately. Clinical trials consistently demonstrate reduced mortality rates among compliant individuals. Physicians monitor lipid profiles regularly to ensure therapeutic targets are met. Side effects rarely outweigh the substantial cardiovascular benefits observed. Muscle pain complaints sometimes arise but alternative statins exist readily. Adherence to medication schedules prevents dangerous spikes in particle counts. Revascularization procedures like PCI serve as backup options when meds fail. Angioplasty opens the narrowed vessel lumen mechanically with balloons. Stent placement keeps that artery patent against further constriction attempts. Bypass grafting offers a durable route for severe multi-vessel blockage cases. Early detection combined with aggressive management saves the most lives globally.
Philip Wynkoop
1 April 2026 - 09:47 AM
I agree completely with this information.
Tommy Nguyen
3 April 2026 - 05:08 AM
glad someone finally said it simple and clear without the confusing words. prevention is definitely key here and people need to move more.
Paul Vanderheiden
3 April 2026 - 21:23 PM
I heard about your loss and Im so sorry that happened to your family. Losing a parent is always hard especially with heart issues like this. There are so many ways to stay strong now that medicine has improved a lot. Keep moving forward and focus on what you can control in your own life today. You are not alone in this fight and there is hope for longevity.
Jeannette Kwiatkowski Kwiatkowski
4 April 2026 - 00:18 AM
most people here dont understand the complexity of metabolic syndrome anyway so this advice goes over their heads. true wellness requires a certain level of discipline that casual readers lack entirely. we see the same excuses repeated constantly about diet and exercise habits. the smart ones follow the guidelines while the rest just wait for surgery appointments.
Kameron Hacker
5 April 2026 - 20:28 PM
This assertion regarding discipline ignores socioeconomic barriers affecting access to care fundamentally. Blaming patients for outcomes disregards systemic failures in public health education policies. Your perspective suggests a lack of awareness regarding resource allocation disparities in medicine. It is essential to maintain empathy rather than judging individual adherence capabilities harshly. Scientific data supports the idea that environment drives behavior far more than willpower does.
Jordan Marx
6 April 2026 - 01:42 AM
The Ankle-Brachial Index really offers valuable systemic vascular insight beyond local heart symptoms. Clinicians often overlook peripheral artery disease coexistence during standard cardiac workups. Evaluating ABI ratios provides a clearer map of endothelial dysfunction throughout the body. A systolic pressure differential greater than thirty millimeters indicates significant stenosis risk. Incorporating this simple metric helps stratify high-risk cohorts accurately for preventative interventions. Peripheral pulse checks should be routine whenever CAD suspicion arises clinically. Holistic assessment improves prognostic modeling substantially for long-term survival metrics. Patients benefit immensely when physicians look past isolated coronary anatomy findings.
Devon Riley
7 April 2026 - 20:59 PM
Knowing about those extra tests gives peace of mind to families worried about hidden risks 💪❤️. Its good to see doctors using all available tools to catch problems early. Technology has come so far since previous generations lost loved ones unexpectedly. Every bit of data helps protect the heart muscle from future damage. Stay positive and keep asking for the right diagnostics always 🩺✨.
Sophie Hallam
9 April 2026 - 11:25 AM
Risk factors vary widely depending on genetics and environment both equally important. Understanding personal history helps tailor appropriate screening protocols accordingly. Smoking cessation programs remain crucial regardless of how much time passed since quitting. Social determinants of health play a significant role in overall population outcomes. Thank you for sharing this detailed overview of modern diagnostic approaches.
kendra 0712
10 April 2026 - 22:49 PM
This is such important info!!! The detail about statin mechanisms is super helpful! I will definitely share this with my mom! Prevention is key!!!! Medication compliance saves lives! We all need to listen closely! Thanks for writing this out!!
Richard Kubíček
11 April 2026 - 00:41 AM
Living with chronic conditions requires a mindset shift towards stewardship of the self rather than victimhood. Modern medicine treats symptoms while ancient wisdom focused on balance and harmony within the vessel walls. The intersection of cardio-oncology shows how interconnected bodily systems truly are over a lifetime. Investing in prevention reflects a philosophical commitment to remaining active for longer durations. We must view health as a continuous spectrum rather than a binary pass fail scenario. Small daily habits accumulate into massive differences in outcome trajectories decades later.